JBRA Assist. Reprod. 2022;16(01):19-22
ARTIGO ORIGINAL
doi: 10.5935/1518-0557.2012.16.1.03
Urinary human chorionic gonadotropin to trigger final oocyte maturation: 5000 X 10000 IU - is there any difference?
Urinary human chorionic gonadotropin to trigger final oocyte maturation: 5000 X 10000 IU - is there any difference?
Instituição: ORIGEN, Centro de Medicina Reprodutiva, Belo Horizonte /MG
RESUMO
Objetivo: Comparar os resultados de ciclos de Fertilização in vitro (FIV) com o uso de diferentes doses (10000 IU e 5000 IU) de gonadotrofina coriônica humana urinária para desencadear a maturação oocitária.
Métodos: Este é um estudo prospectivo, observacional com 108 pacientes em ciclos de FIV, que apresentavam mais de 15 folículos com um diâmetro >17mm, obserrados no dia da administração do hCG. Os 2 grupos de comparação foram definidos de acordo com as doses de hCG administradas ~36 horas antes da punção ovariana: Grupo 1 (10 000 IU) e Grupo 2 (5000 IU), em um protooolo longo de hiperestimulação ovariana.
Resultados: Grupo 1 teve 74 pacientes (idade media 33,46±3,9) e o Grupo 2 teve 34 pacientes (idade media 32,43±5,4). Todas as pacientes foram submetidas à punção ovariana com mais de 15 folículos. Os níveis de estradiol no dia da administração do hCG foram 3567±620 no Grupo 1 e 4060±730 no Grupo 2, p=0,38. O númeeo médio de oócitos maduros foi de 15,21±3,7 (Grupo 1) e 21,4±5,22 (Grupo 2), p<0,001. Não houve diferença significativa entre os grupos com relação às taxas de gestação clínica, gestação em curso, abortamento e na incidência de sindrome de hiperestímulo ovariano grave.
Conclusão: Observamos que o uso de uma dose menor de hCG urinário (5000 IU) ao invés da dose tradicional (10000 IU) usada para induzir a maturação oocitária final, parece não afetar negativamente os resultados de FIV e a incidência de sindrome de hiperestimulo grave não foi diferente.
Keywords: urinary human chorionic gonadotropin, hCG dose, oocyte maturation, ovarian hyperstimulation syndrome
INTRODUCTION
The human chorionic gonadotropin (hCG) is used in controlled ovarian hyperstimulation (COH), to replace the endogenous LH surge and simulates its physiologic effects to induce final follicular and oocyte maturation (Wang et al, 2011). HCG is a heterodimeric hormone belonging to glycoprotein hormone and cystine-knot growth factor families and it is a natural analogue of LH. Both LH and hCG interact with the same receptor (LH/hCG receptor) and this interaction is associated with the initiation and maintenanne of pregnancy (Filicori et al, 2005; Lapthorn et al, 1994). The events consequents of the LH rising on the follicular phase in natural cycles, can be reproduced by the use of hCG in IVF cycles. The reproduction of these events is essential to the treatment success. The main effects of the LH rising are: the final oocyte maturation, oocyte dissociation from the follicular wall and the corpus luteum formation. The hCG represents an efficient form of subssituting the LH activity, because the both hormones binds to the same receptor and exerts similar functions. In in vitro fertilization (IVF) treatments, we can use the urinary hCG (u-hCG) or the recombinant hCH (r-hCG) for final oocyte maturation (Filicori et al, 2005; Kolibianakis et al, 2007; Driscoll et al, 2000).
HCG circulating half -life is greater than 24 hours, which is longer than the LH"s (approximately 60 minuues), and persists up to 6 days after ovulation. The hCG has a higher affinity to the receptor and a lower clearence than the LH. It simulates the LH rising and induces reactivation of oocyte meiosis (Tsoumpou et al, 2009; Saleh et al, 2007). The hCG is either imporrant in the early stages of pregnancy. It also seems to have beneficial effects in uterine receptivity by the stimulation of the endometrial growth and maturation, and either interacts with the LH/hCG receptors in the endometrium promoting the maintenance of the corpus luteum (Tsoumpou et al, 2009; Licht et al, 2003).
Despite having a key role in the controlled ovarian stimuuation treatments, the hCG is also associated with deveeopment of ovarian hyperstimulation syndrome (OHSS). OHSS is an iatrogenic complication of the COH during assisted reproductive technology (ART). It may occur during the luteal phase or during the early pregnancy. It almost always occurs during the ART, but it may occur during treatments with the use of clomiphene citrate and even in a spontaneous pregnancy (Delvigne, 2009; Nastri et al, 2010; Delvigne, 2002; Michaelson-Cohen, 2008). The real incidence of OHSS is difficult to determine, because the different studies report different incidences, according to the classification that is used to classify the OHSS. But, the incidence of moderate and severe OHSS are estimated to be between 3 to 6% and 0.1 to 3%, respectively (Delvigne, 2009; Nastri et al, 2010).
There are different doses of u-hCG that can be used to trigger the final oocyte maturation, ranging from 3000 IU to 25000 IU, but the optimal dose is not well established (Tsoumpou, 2009; Nargung, 2007). There are some studies in animals demonstrating that the hCG dose necessary for ovulation is higher than that necessary for oocyte maturation (Schmidt, 2004). Therefore, as in the IVF treatment the use of hCG is necessary only to the oocyte maturation and not to induce the ovulation, it can be postulated that the u-hCG dose required would probably be lower than the dose normally used (10000 IU).
The purpose of this study was to compare the results of IVF cycles, including the number of mature oocytes retrieved, clinical pregnancy rate, ongoing pregnancy and the incidence of severe OHSS, using different doses (10000 IU e 5000 IU) of u-HCG for triggering final oocyte maturation. We hypothesized that the dose of 5000 IU would be adequate for the final oocyte maturation.
MATERIALS AND METHODS
This was a prospective observational study to assess the hypothesis that using a lower dose of u-hCG (5000 IU versus 10000 IU) for final oocyte maturation would not decrease the IVF outcomes and could lower the risk of severe OHSS. The study was designed in a private assisted reproduction center (Clínica Origen - Rio de Janeiro - Brasil).
The inclusion criteria were as follows: 1) first IVF cycle; 2) age < 38 years; 3) serum day 3 FSH levels < 10 IU/L and E2 < 80 pg/mL; 4) absence of endometriomas detecced at ultrasound; 5) more than 15 follicles with a mean diameter of 16 mm, seen on ultrasound on the day of hCG administration. The exclusion criteria were as follows: 1) age >= 38 years; 2) serum day 3 FSH levels >= 10 IU/L; 3) patients who did not undergo their first IVF treatment; 4) patients who were coasted more than two days; 5) severe male factor infertility (< 5 million motile spermatozoa/mL and/or requiring testicular sperm extraction). Ovarian stimulation consisted of a long protocol for ovarian stimulation. For pituitary down-regulation, patients were treated with a GnRH agonist depot, administred SC on day 21 of the menstrual cycle. All patients were evaluated after 10 days of agonist administration with serum estradiol levels and transvagiial sonography. When pituitary down-regulation was confirmed (no follicles > 10mm present and serum estradiol levels < 80 pg/mL) hMG or recombinant FSH were given in a step-down protocol. Serial ultrasound examinations and serum E2 levels were used to assess ovarian response, and to adjust the gonadotropin dose. The patients received a trigger dose of either 10000 IU or 5000 IU of purified urinary hCG when at least 3 follicles reached 17mm diameter.
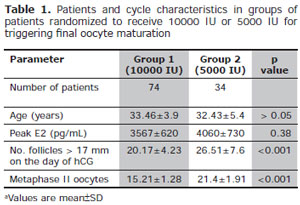
Table 1. Patients and cycle characteristics in groups of patients randomized to receive 10000 IU or 5000 IU for triggering final oocyte maturation
Oocyte retrievals were performed ~36 hours after hCG administration and ICSI was performed in all cases. All patients received luteal phase support with vaginal progesterone starting the day after oocyte retrieval and continued up 12 weeks of pregnancy. Embryo transfer was performed 48-72 hours after oocyte pick-up.
Comparisons between the two groups were made for: age, estradiol levels on the day of hCG administration, the number of mature oocytes retrieved, clinical preggancy rates, ongoing pregnancy rates, miscarriage and the incidence of severe OHSS. Clinical pregnancy was considered as the presence of gestational sac with fetal heart activity, as assessed by ultrasound at 7 weeks of gestation. Ongoing pregnancy was defined as pregnancy progressing beyond the 12th gestational week.
Data were expressed as mean±SD. P<0.05 was consiiered statistically significant. The normality of distribuuion of variables was tested with Kolmogoroff-Smirnoff test. Independent sample t-test was used for continuous variables wich were normally distributed and Mann-Whittey U test for data not normally distributed. Chi-squared test with Yates correction or Fisher exact test was used for qualitative variables. The Statistical Package for Social Science (SPSS, version 17.0 for windows; SPSS Inc., Chicago, IL) was used for data analysis.
RESULTS
The patient and cycle characteristics of the groups randomized to receive 5000 or 10000 IU of hCG for triggering final oocyte maturation are shown in Table 1. There were no statistically significant differences regarring demographic characteristics among the groups. The E2 levels on the day of hCG administration, the mean number of follicles > 17mm on the hCG day and the mean number of mature oocytes retrieved are shown. The number of follicles and the number of matuue oocytes retrieved were statistically significant different. Group 1 (10000 IU hCG) had 20.17±4.23 follicles and group 2 (5000 IU hCG), 26.51±7.6 (p=0,0001).
Among mature oocytes retrieved, the media in group 1 was 15.21±1.28 and in group 2, it was 21.4±1.91. Table 2 and Figure 1 show the IVF outcomes of the two groups with respect to the clinical pregnancy rates, ongoing pregnancy rates, miscarriage and frequency of OHSS. There was no statistically significant difference between the groups in the clinical pregnancy rate (Group 1, 55.4%; Group 2, 52.94%; p = 0.81), ongoing pregnancy rate (Group 1, 50 %; Group 2 47%; p=0.77) and miscarriage (Group 1, 9.7%; Group 2 11,1%; p=0.87). Severe OHSS occurred in two patients (2,7%) in the Group 1 and in two patients (5,7%) in the 5000 IU group with no statistically significant difference (p=0.41). Severe OHSS occurred in two patients (2,7%) in the 10000 IU group and in two patients (5,9%) in the Group 2, with no statistically significant difference (p=0.41).
DISCUSSION
This prospective study suggests that there are no signifiiant differences in IVF outcomes, when comparing 10000 x 5000 IU of u-hCG to trigger final oocyte maturation in IVF cycles in high responder patients treated with a long protocol for ovarian hyperstimulation. Despite some differences in the number of mature oocytes retrieved (more oocytes retrieved in the lowest dose), the pregnancies rates were not different between the two groups. Also the incidence of severe OHSS was similar in the two groups. Currently, there are some studies that have compared different doses of hCG for triggering final oocyte maturation and cycle outcomes. But it has not been established the ideal dose to be used. There are different results and comparisons among the studies. Tsoumpou et al. conducted a systematic review in order to establish the ideal dose of u-hCG to trigger final oocyte maturation without increasing the inciience of OHSS. They concluded that the dose of hCG should be individualized. Good responders do not need to receive higher doses than 5000 IU, whereas poor responders would benefit from higher doses of HCG. A meta-analyses was not feasible due the insufficienty number of studies assessing the same outcome and significant heterogeneity (Tsoumpou et al, 2009).
It could be expected a decrease in the number of oocytes recovered, in the number of mature oocytes and in the fertilization rates with the use of a lower dose of u-hCG (Kolibianakis et al, 2007). Abdalla et al analyzed the effects of 2000 IU, 5000 IU and 10000IU . When 2000 IU of hCG was used for final oocyte maturation, lower number of oocytes were retrieved comparing with the group that received 5000 IU or 10000 IU but there was no significant difference in pregnancy rates. They concluded that the lowest dose of hCG that should be used is 5000 IU (Abdalla et al, 1987). In a prospective study, Wikland et al. found no difference in the number of mature oocytes, pregnancy rates (PRs), and delivery rates when 5000 IU hCG and 10000 IU hCG were used. There was no statistically difference in the live birth rate when comparing the groups receiving 5000 or 10000 IU (Wikland et al, 1995). Prien et al. compared the cliniial outcomes of final oocyte maturation with 5000 IU or 10000 IU of u-hCG. There was no difference on the oocyte recovery and PRs (Prien et al, 2000).
In our study, we had different results when the number of oocytes retrieved was analyzed. The group that received the lowest dose of hCG had more mature oocytes, but this same group had more follicles up to 15 mm in the day of hCG administration. This is in accordance with the study of Detti et al. In a retrospective cohort study in antagonist cycles, they compared the use of 5000 IU, 10000 IU and 15000 IU and observed the higher number of oocytes retrieved in the group of highest levels of estradiol in whom the lowest doses of u-hCG were administred (Detti et al, 2007).
Schimidt et al retrospectively evaluated the use of different doses of hCG (3300 IU versus 5000 IU) in high responders patients submitted to a long protocol of ovarian stimulation and the use of urinary gonadotrooins. The different doses were given based on E2 levels on the day of final oocyte maturation. There were no differences between the groups in the percentage of mature oocytes, biochemical pregnancy and clinical pregnancy (Schmidt et al, 2004).
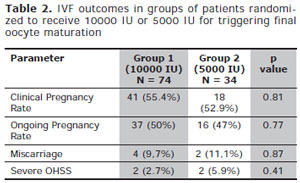
Table 2. IVF outcomes in groups of patients randomiied to receive 10000 IU or 5000 IU for triggering final oocyte maturation
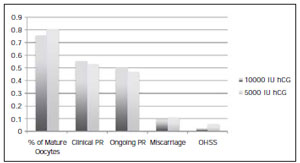
Fig. 1. IVF outcomes in patients receiving 10000 IU of hCG versus 5000 IU of hCG
In a randomized controlled trial, Kolibianakis et al compared the use of 2500 IU, 5000 IU, and 10000 IU in antagonist cycles in women with polycystic ovarian syndrome. They demonstrated that a decrease in the dose of hCG up 2500 IU can be used without modifying the results in terms of oocyte recovery and ongoing pregnancy rate (Kolibianakis et al, 2007).
HCG may have some adverse effects due to its long half-life. One of this is an increased risk to develop the OHSS. The incidence of OHSS in cycles using different doses of u-hCG was studied by Schimidt et al. and Kolimianakis et al. and they found no difference in the inciience of OHSS reducing the dose of u-hCG administred (Kolibianakis et al, 2007; Schmidt et al, 2004). This is in accordance with our study, where we did not find differences in severe OHSS despite the dose of u-hCG. But the sample size was not big enough to show a conclusive result. Considering that the incidence of severe OHSS in IVF cycles ranges from 0,1 to 3% of all cycles, it would be necessary at least 4131 patients in each group of patients to show that by lowering the u-hCG dose, the incidence is decreased by 1%. So, it would not be feasiile to conduct a single study with this amount of patient (total number of 8262) trying show a significant difference in the incidence of OHSS with diferent doses of hCG. Patients with OHSS remain a challenge in the ART. It is important to try to identify the risk patients and have a close segment of these patients. Currently, with the GnRH antagonist protocol, we can avoid the use of the hCG in the high risk patients using the GnRH analooue to induce the final oocyte maturation and oocyte or embryo cryopreservation, eliminating the risk of the development of early or late OHSS in these patients.
We need more robust randomized trials to have a definition of the ideal dose of u-hCG to be administred for final oocyte maturation. But we can suggest with this study and other studies available in the literature that the use of 5000 IU of u-hCG instead of the traditional dose of 10000 IU would not negatively affect the IVF outcomes.