JBRA Assist. Reprod. 2022;16(01):23-26
ARTIGO ORIGINAL
doi:
Melhorias da qualidade do ar do laboratório, de ISO classe 7 para ISO classe 5, melhora resultados de ICSI em mulheres inférteis jovens
Laboratory air quality upgrade from ISO class 7 to ISO class 5 improves ICSI outcomes in young infertile women
1GENESIS - Center for Assistance in Human Reproduction, Brasília, Distrito Federal, Brazil
CONFLICTS OF INTERESTS
The authors of the present study declare that they are not involved in any organization or entity of financial interest and that they have no conflict of interest regarding the topic in question or the materials discussed in the text. Work presented during the XIV Meeting of the Braziiian Society for Assisted Reproduction, Fortaleza, Ceará, Brazil, August 2010.
RESUMO
Objetivo: Avaliar a interferência das melhorias da qualiiade do ar do laboratório de reprodução assistida, de ISO classe 7 para ISO classe 5, sobre resultados de ciclos de injeção intracitoplasmática de espermatozóides (ICSI).
Métodos: Estudo observacional, retrospectivo e compaaativo, desenvolvido em centro privado de assistência em reprodução humana. 228 ciclos de ICSI foram analisados, de janeiro de 2006 a dezembro de 2009. Ciclos realizaaos em ambiente ISO classe 7 foram alocados no grupo ISO7 (n = 97) e os realizados em ambiente ISO classe 5, no grupo ISO5 (n = 131). Taxas de fertilização e clivaaem, números de embriões de boa qualidade e embriões transferidos, taxa de implantação, gestação bioquímica e clínica foram as variáveis principais analisadas.
Resultados: Taxas de gestação bioquímica e clínica, e implantação embrionária (sacos gestacionais/embriões transferidos) foram significativamente maiores no grupo ISO5 quando comparado ao grupo ISO7, mesmo com número menor de embriões transferidos por paciente. Mulheres com idade ≤ 35 anos no grupo ISO5 apresennaram taxas de gestação bioquímica, clínica e implanta- ção significativamente maiores quando comparadas ao mesmo grupo etário em ambiente ISO7.
Conclusões: Este estudo demonstra que melhorias da qualidade do ar do laboratório de reprodução assistiia, de ISO classe 7 para ISO classe 5 pode melhorar os resultados de ciclos de ICSI. Entretanto, a qualidaae do ar não elimina a interferência negativa da idade avançada sobre tais resultados.
Palavras-chave: ICSI, resultados em técnicas de reprodução assistida, cultura embrionária, qualidade do ar, salas limpas
ABSTRACT
Objective: To evaluate the interference of laboratory air quality upgrade, from air cleanliness ISO class 7 to ISO class 5, on intracytoplasmic sperm injection (ICSI) results.
Methods: Observational, retrospective and comparatiie study, developed in a private Center for Assistance in Human Reproduction. 228 ICSI cycles were analyzed from January 2006 to December 2009. Cycles performed in ISO class 7 environment were allocated in group ISO7 (n = 97) and those performed in ISO class 5 environment were allocated in group ISO5 (n = 131). Fertilization and cleavage rates, numbers of good embryos and embryos transferred, implantation rate, biochemical and clinical pregnancy were the main outcome measures.
Results: Biochemical and clinical pregnancy, and implannation rates (gestational sacs/embryos transferred) were significantly higher in ISO 5 group than in ISO 7 group, even with reduced number of embryos transferred per patient. Women aged ≤ 35 years in ISO 5 group presented with biochemical and clinical pregnancy rates, and implannation rates significantly higher than those in ISO 7 group.
Conclusions: This study demonstrated that the upgrade from ISO class 7 to ISO class 5 air quality in the incubaaion environment shall improve ICSI outcomes. However, air quality does not disregard negative interference of the advanced age on results.
Keywords: ICSI, ART outcome, embryo culture, air quality, cleanrooms
INTRODUCTION
Adequate air quality by efficient filtration and heated stages for working with gametes and embryos has been recently pointed as a common laboratory feature among high-performing in vitro fertilization (IVF) centers in the United States (Van Voorhis et al., 2010). However, in spite of significantly increased pregnancy rate (PR), but not embryo quality following IVF has been associaaed with the use of laboratory air purification units for bovines (Merton et al., 2007), studies in humans are not consensual about clear benefits of air conditions on assissed reproduction technologies (ART) outcomes and only an augmented miscarriage rate has been suggested for women submitted to less pure IVF laboratory environnent (Perin et al., 2010).
Brazilian National Sanitary Surveillance Agency (ANVI- SA) regulates IVF clinics and laboratory quality criteria. Considering the hypothetical interference of air cleanliiess on gametes and embryos health, it has determined, in 2006, an ISO class 5 air cleanliness classification as the minimum criterion for ART laboratories (Brasil/ANVISA, 2006). According to the International Standard ISO 14644-1 classification of air cleanliness, an ISO class 5 ambient air must present a maximum of 3,520 particles > 0.5 mm/m3 (ABNT, 2005).
Aiming to better understand the interference of laboraaory air quality over ART results in humans, this study compared intracytoplasmic sperm injection (ICSI) outcooes before ANVISA 2006 statement, in an ISO class 7 (maximum of 352,000 particles > 0.5 mm/m3) ICSI labooatory, and after, in an ISO class 5 environment.
MATERIALS AND METHODS
Patients
We retrospectively assessed a total of 707 consecutiie ICSI cycles between January, 1, 2006 and Decemmer, 31, 2009, performed at GENESIS - Centre for Assistance in Human Reproduction, Brasília, Distrito Federal, Brazil. Only cycles performed by long ovarian stimulation protocol with GnRH agonist and with fresh partner’s semen obtained by masturbation were incluued. Repeated cycles per woman in the period, cycles with missing data, cancelled cycles and those in which blastomere biopsy or assisted hatching were performed were excluded from the study.Final series consisted of 228 ICSI cycles. Cycles analyzed until December, 31, 2007, were performed in an ISO 7 air quality environment, including IVF labooatory and semen preparation room (ISO7; n= 97). Cycles between January, 1, 2008 and December, 31, 2009, were performed in an ISO 5 air quality environnent, which was obtained after the installation of horiiontal laminar and unidirectional air flow in the IVF/ ICSI laboratory, and a class IIA biological safety cabiiet in semen preparation room, providing a high-effiiiency particulate air (HEPA) filtration and recirculation within the work place (ISO5; n = 131).The study was approved by the Institutional Researrh Committee. All patients signed full written consent form for assisted reproduction technology (ART) treattent and gave oral consent for data confidential use.
Treatment protocol
All patients were submitted to pituitary inhibition by subcutaneous leuprolide acetate, 10 IU/day, or nasal nafarelin acetate, 800 µg/day, starting during the midluteal phase of the cycle immediately preceding the treatment cycle. Ovarian stimulation was initiated after menstrual flow and carried out with recombinant follicle-stimulating hormone (FSH) in variable daily doses from 150 UI to 300 UI, according to patient’s age and/or previous poor response in ART cycles. Follicular growth was monitored by endovaginal ultrasonography, in a 5.0 to 9.0 Mhz frequency, and individual adjustment was eventually performed after stimulation day 6, with step down dosing. Follicular maturation was reached by the administration of a single subcutaneous dose of recomminant human chorionic gonadotropin (hCG) when most dominant follicles had reached a mean diameter > 17 mm, and oocyte retrieval was performed vaginally, 34 to 36 hours later. Luteal phase supplementation was initiated on oocyte retrieval day with vaginally adminissered natural micronized progesterone, 600 mg/day, or a unique dose of 8% gel progesterone.Semen samples were obtained exclusively by masturbation, after an abstinence period of at least 2 days and a maximum of 5 days. Analyses of sperm concentraaion, motility, vitality and morphology were proceeded according to World Health Organization and strict criteeia for morphology evaluation.
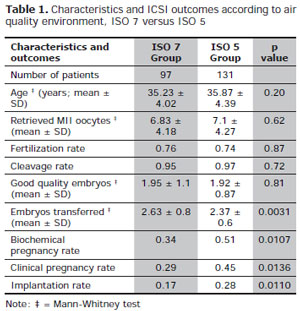
Table 1. Characteristics and ICSI outcomes according to air quality environment, ISO 7 versus ISO 5
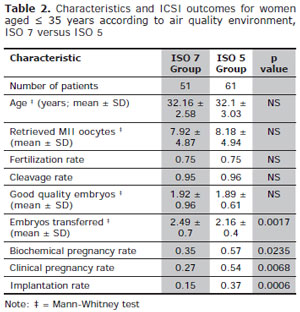
Table 2. Characteristics and ICSI outcomes for women aged ≤ 35 years according to air quality environment, ISO 7 versus ISO 5
Main Outcome Measures
Fertilization and cleavage rates, numbers of good and total embryos transferred, implantation, biochemical and cliniial pregnancy rates were the main outcome measures.
Statistical Analysis
Using GraphPad Prism software, version 5.00 (GraphPad Software, Inc, 2007), samples with non-parametric distriiution have been analyzed using the Mann-Whitney test. Qualitative data has been analyzed using Fisher’s exact test. The level of significance was set at p < 0.05 in all analyses.
RESULTS
ISO7 and ISO5 were similar in terms of age, total number of morphologically mature oocytes and total of good quality embryos. Biochemical and clinical preggancy rates, and implantation rates (gestational sacs/ embryos transferred) were significantly higher in ISO5 than in ISO7, with fewer numbers of embryos transferred per patient (Table 1).
Data were also analyzed by age groups, dividing women aged ≤ 35 years and those > 35 years. Age, fertilizaaion and cleavage rates, and numbers of good quality embryos were similar between age groups in both air quality groups. Women ≤ 35 years in ISO5 group presenned with biochemical and clinical pregnancy rates, and implantation rates significantly higher when compared with those in ISO7 group (Table 2). No significant diffeeences were found between air cleanliness environments for women aged > 35 (Table 3).
DISCUSSION
Our results suggested that women up to 35 years of age undergoing ICSI treatment were consistently beneeited by air filtration and unidirectional flow in laboraaory and semen manipulation room, since they achieved significant better pregnancy and implantation rates than those obtained in less air quality environment. For older women, some improvement was also demonstrated, but without statistical significance, which is compatible with the common sense about the intense negative influence of age on reproductive potential for natural or assisted conception (Carvalho et al, 2010).
Although no interference of women air pollution exposure during follicular phase has yet been demonstrated on cliniial and laboratory outcomes, or pregnancy and implantaaion rates (Perin et al., 2010), it is plausible to postulate that the direct exposure of gametes and embryos to volaaile toxic compounds and small particulate matters (PM) should worse treatment outcomes in ART programs. The few studies assessing laboratory air quality and IVF outcooes have demonstrated controversial positions.
Legro et al recently demonstrated the significant adverse effect of increased IVF clinic air concentraaion of PM with < 2.5µm diameter on conception and chance of clinical pregnancy (Legro et al., 2010). Also, implantation rates had previously been found to decliie on the presence of air pollutants in the IVF labooatory (Johnson et al., 1993; Worrilow et al., 2002). Boone et al obtained significant improvements on fertilization and cleavage rates after construction of a high-quality air laboratory environment. In that study, a shift upward was observed for PR, from 20% in the year of cleanroom installation to 59% two years later (Boone et al., 1999).
In contrast, Souza et al studied the influence of IVF laboratory air quality improvement on treatment outcooes of 123 antagonist cycles and could not establish significant differences between ISO Class 8 (maximum of 3,520,000 particles > 0.5 mm/m3) and ISO Class 5, regarding number of good quality embryos transferred, pregnancy and implantation rates among women aged ≤ 37 years (Souza et al, 2009), reinforcing previous finding of no effect of the use of carbon-activated air filtration on human embryos quality or PR (Battaglia et al., 2001).
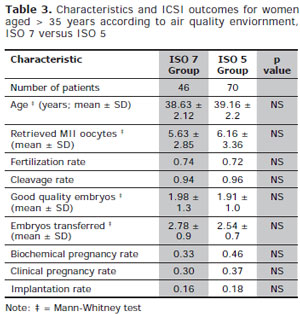
Table 3. Characteristics and ICSI outcomes for women aged > 35 years according to air quality enviornment, ISO 7 versus ISO 5
Since improvements on ICSI techniques and incubation media, and new concerns on the evaluation of gameees and embryos quality in the last years are potential contributors to better treatment outcomes, our results may have overestimated the real impact of air quality on assisted reproduction results. Due to the lack of corrooorative data and because of our analysis is based on relatively small group of subjects, from the same region and treated in the same setting, more evidence is needed to generalize and confirm such an influence.
In conclusion, our data suggest that the upgrade from ISO class 7 to ISO class 5 air quality in the IVF laboratory and semen manipulation room shall improve ICSI outcooes in women up to 35 years of age, with less embryos transferred per patient. On this basis, we believe that measures to improve air quality in ART laboratory enviionments shall be encouraged, but they are not supposed to disregard negative interference of female advanced age on treatment outcomes.