JBRA Assist. Reprod. 2012;16(06):337-342
ARTIGO ORIGINAL
doi: 10.5935/1518-0557.2012.16.6.05
Experimental evaluation of bovine pericardium efficacy on adhesion pelvic prevention in the dog model
Avaliação experimental da eficácia do pericardio bovino na prevenção de aderências pélvicas em modelo canino
1Department of Gynecology and Obstetrics, School of Medicine (Laboratory of Human Reproduction), Federal University of Goiás - UFG - Goiania (GO), Brazil
2Plastic Surgeon. Former Resident in the Department of Surgery, Federal University of São Paulo - School of Medicine-UNIFESP - São Paulo (SP), Brazil
3Department of Gynecology, Federal University of São Paulo - School of Medicine - UnIFESP - São Paulo (SP), Brazil
4Department of Gynecology, Federal University of São Paulo - School of Medicine - UnIFESP and in the Faculty of Medicine, University of São Paulo - USP - São Paulo, Brazil
Department of Gynecology and Obstetrics and Department of Surgery (Experimental Surgery), Faculty of Medicine, Federal University of Goiás; Department of Gynecology, Federal University of São Paulo - School of Medicine.
ABSTRACT
Purpose: to investigate the efficacy of bovine pericardium to prevent pelvic adhesion in dogs.
Methods: Seventeen female non pregnant dogs were anesthetized and submitted to two adhesion-inducing lesions - the first lesion was performed in the anterior portion of uterus (elliptical incision) and sutured with an ischemic line of chromic catgut and the second, when closing the peritoneum, also with an ischemic suture. BP was used as the barrier agent in nine dogs, fully covering the first lesion and applied on the inferior part of the second lesion. Six days later, the dogs were sacrificed and the adhesions were examined according to the ¨More Comprehensive Adhesion Score Method¨ (MCASM, Adhesion Study Group-EUA) and to the score developed by the author in which only the percentage of the adhesion is examined, ¨Adhesion Extension in Experimental Lesion¨ (AEEL).
Results: There were no significant differences between the two groups regarding weight and surgical time in minutes . no significant differences were observed between the MCASM scores of the two groups (6.50 vs. 6.00, p= 0.718) and the AEEL (4.87 vs. 4.33, p=0.615) for lesion 1. There were significant differences in the second lesion in the two groups, regarding the mean scores given by the MCASM system (4.62 vs.7.55, p=0.005) and the adhesion extension score (2.75 vs. 4.77, p=0.015).
Conclusions: BP did not prevent the formation of adhesions caused by the lesions performed. Furthermore, BP enhanced the formation of adhesions in lesion 2.
Key words: Postoperative adhesion prevention, surgical barriers, bovine pericardium, experimental lesions of adhesion, prevention of adhesion.
RESUMO
Objetivo: avaliar a eficácia do pericárdio bovino (PB) na prevenção de aderências em cães submetidos a duas lesões indutoras de aderências no grupo controle (GC) e no grupo experimental (GE).
Métodos: dezessete cadelas, sem raça definida e não prenhas, foram anestesiadas e submetidas a lesões indutoras de aderências, sendo a primeira a miometrectomia anterior com sutura isquêmica, e a segunda, o fechamento do peritônio com sutura ancorada isquêmica. no GE, com nove cadelas, colocou-se o PB recobrindo integralmente a primeira lesão; na segunda lesão, recobriu-se a área de sutura isquêmica na extremidade inferior. Após seis dias, no mínimo, as cadelas foram sacrificadas e as aderências quantificadas, segundo a sistematização sugerida pela Adhesion Sudy Group denominada MCASM*(more comprehensive adhesion score method), e pela avaliação do percentual de área aderida, excluindo a força da aderência, denominada AEEL*(adhesion extension experimental lesion).
Resultados: O GC e GE não tiveram diferenças significativas na média de peso (kg) e tempo cirúrgico em minutos (12,62/15,66 p= 0, 3868) e (78,25/77, 88, p= 0, 9086). Lesão 1: o GC apresentou escore médio 6,50 versus 6,00 no GE, p= 0,718 (MCASM) e 4,87/4,33 com p= 0,615 (AEEL), diferenças não significativas. Lesão 2: o GC teve escore médio 4,62 versus 7,55 no GE e p= 0,005 (MCASM) e 2,75/4,77 com p= 0,015 (AEEL), diferenças significantes.
Conclusões: As lesões foram fortes indutoras de aderências, e o PB não preveniu a formação de aderências. Além disso, o PB produziu mais aderências na lesão 2.
Palavras-chave: aderências pós-operatorias, métodos de barreira cirúrgicos, pericárdio bovino, lesões experimentais de aderências, prevenção de aderências.
ACKNOWLEDGEMENT
This work was carried out at the discipline of Operative Technique and Experimental Surgery in the Department of Surgery, Faculty of Medicine, UFG, with the participation of gynecologists: Vidal Augusto Cortizo, Denis Ribeiro de Oliveira, José Hidalgo Donizeth, Vinicius Alves Oliveira and residents of the Department of Surgery, Faculty of Medicine, UFG and Department of Surgery, Paulista School of Medicine(UnIFESP), and medical students.
INTRODUCTION
Over the past years abdominopelvic adhesion has been studied in a very detailed and professional way. These studies analyze the importance of adhesion formation to the human being once it is related to chronic pelvic pain, infertility, surgery complication in reoperation and the relevant costs in the health care systems.
Ellis et al., 1999 studied the percentage of hospital admittance caused directly or indirectly by abdominopelvic adhesion in Scotland in the year of 1994. The studied population consisted of patients that underwent surgery in 1986 who had no record of abdominopelvic surgery in the preceding 5 years. Among 27.790 patients 34.6% were readmitted to hospital on an average of 2.1 times in ten years of observation; 22.1% of patients were readmitted in the first year after the surgery. In developed countries the main cause of bowel obstruction can be attributed to abdominopelvic surgery (Beck et al., 2000).
Svanes Fevang et al., 2004 studied 500 patients in norway between 1961 and 1995 . They underwent surgery because of bowel occlusion related to adhesion and they were followed for an average of ten years, but some patients were followed for fourty years. The cumulative recurrence rate was 18% at ten years and 29% at thirty years. Patients with high recidivism rate showed higher recurrence rate and for those who underwent four previous surgeries, for example, the recidive rate was 81%. Wilson et al., 2002 estimated that in Scotland the re-admission cost for post-surgical abdominal adhesion, mainly colon-rectal, during ten years follow-up observation was about 569 million pounds. Scientists speculate that if adhesion prevention products costing 50 pounds per patient were used, the hospital re-admittance would diminish 16% and if the cost was 200 pounds the hospital re-admittance would diminish 64% in three years.
The barrier method presents preventive properties against adhesion and this method is the most well researched over the past years. Among the common barrier methods, apparently effective, there is the polytetrafluoroethylene membrane (PTFE) commercialized by Gore Tex Surgical Membrane, Interceed and Seprafilm. Many multicentre studies were published about Interceed (oxidized regenerated cellulose and Absorbable Adhesion Barrier) after studies in animals (Interceed Adhesion Study Group, 1998; nordic Adhesion Prevention Study Group, 1996; Franklin, 1995). Such studies showed a reduction in the incidence, extension and severity of post-surgery adhesion in human patients but, on the other hand, some negative results were showed by different researches (Saravielos & Li, 1996; Reid et al.,1997; Baysal, 2001). Diamond & The Seprafilm Adhesion Study Group., 1996 showed positive results of Seprafilm (sodium hyaluronate-carboxymethylcellulose membrane) against pelvic adhesion.
Boyers et al., 1988 studying the effect of the expanded membrane (PTFE) in rabbits achieved a positive result. This result motivated a multicentre study in humans which was published in 1992 by The Surgical Membrane Study Group. They tested the effectiveness of the membrane against adhesion reformation. After this study some conclusions could be drawn: a-few training procedures are needed; b-the membrane must be located at least 1cm beyond the cruenta area; claparoscopic removal was not a difficult task; d-the product did not cause the death of the user. Studies in animals (Montz et al., 1992; Grow et al., 1994; Hellebrekers et al., 2000) showed the positive adhesion prevention effect of Gore Tex Surgical Membrane. Other authors (Haney et al., 1995; The Miomectomy Adhesion Multicenter Study Group, 1995) confirmed this positive result in humans. Hurst et al., 1999 coordinated an observational multicentre study to determine if permanent implantation of the PTFE membrane in the pelvis caused any adverse effects and they concluded that removal of the barrier was not necessary. The membrane was implanted permanently and no long-term complications occurred in any of the 146 women subjected to the study.
Farquhar et al., 2006 conducted a metanalysis study to assess the effect of mechanical barriers such as PTFE membrane, Interceed and Seprafilm. Their results suggest a positive adhesion prevention effect and Gore-Tex may be slightly superior to Interceed in preventing adhesion.These products are expensive in our country and it has motivated scientists to look out for different options which would be compatible with our environment and less expensive. In our country the bovine pericardium(BP) is intensively used in heart surgery and that could be the right option. Such membrane is stored in formaldehyde and it is thicker than the Surgical Membrane which could be an inconvenience. On the other hand the bovine pericardium is resistant and malleable (Braile et al., 1998). Mavritas et al., 2005 , studied the dynamic mechanical behavior of BP in its native form and under specific enzymatic degradation with chondroitinase ABC. They confirmed the viscoelastic properties of BP.
Gomes et al., 1994 studied the effect of this product in abdominal hernias correction in pigs and there was no adhesion formation. Therefore we decided to evaluate the bovine pericardium in adhesion prevention in female dogs with no specific pedigree. An efficient adhesion inducing model was used and it was previously tested in a pilot project approval by Animal and Human Research Ethics Committee in Clinical Hospital of Federal University of Goiás.
METHODS AND MATERIALS
Twenty non-pregnant female dogs with no specific pedigree were assigned to two groups each containing ten animals - control group (CG) and experimental group (EG). For the CG were used only the lesions described as it follows, no anti-adhesion method was used. For the EG, bovine pericardium was used.
In order to induce adhesion formation two lesions were performed. The first lesion consisted of one elliptic incision of 3 to 4 centimeters (Figure 1) in the anterior portion of uterus sutured with an ischemic line of chromic catgut 00 and associated with obliteration to the bilateral uterine artery branch. The second lesion consisted at the closing of peritoneum also with an ischemic suture of chromic catgut 00 (Figure 2). It was performed after placing the bovine pericardium in the animals from EG and at the end of the surgery for the CG.
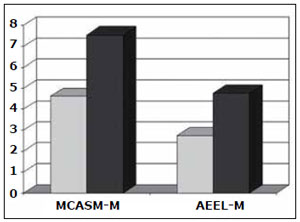
Figure 1. Lesion of the uterus (UL). Elliptical resection and ischemic suture of the anterior uterine portion. Placement of bovine pericardium, covering to the lesion and subsequent fixation of the edges laterally.
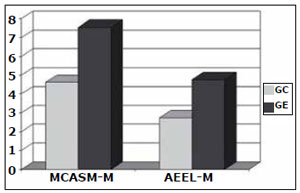
Figure 2. Midline lesion (MLL). Infra umbilical laparotomy showing the placement of bovine pericardium and its laterally fixation to the aponeurosis, covering the midline ischemic peritoneal suture.
The bovine pericardium was fixed to the anterior portion of uterus with six mononylon 5-0 stitches covering the lesion completely. When closing the abdominal wall, the same membrane was used to protect the inferior part of the incision which was 6 centimeters long. The suture was performed in the paramedian aponeurosis by six stitches, three in each side of the suture.
Before the surgery the dogs were observed for three days. They were sanitized a day before the surgery which was performed always in the morning. After the weight evaluation, the animals were anesthetized by a veterinarian who is a Surgery Techniques professor. Intramuscular Acepromazine 1% was used as pre-anesthetic (0,2 ml/Kg-0,5 ml/Kg). Intravenous administration of sodium thiopental 2,5% ( 25mg/ ml) was used as anesthetic with spontaneous breathing. Intramuscular ketoprofene 50mg was used after the surgery every 12 hours for two days. During the surgery days there were an average of five teams with a gynecologist and resident or student as auxiliaries. Six days after the surgery the animals were sacrificed using an intravenous injection of potassium 10% and then re-operated systematically. The animals that died before the sixth day were evaluated for adhesion prevention according to established criteria. In order to evaluate adhesion, a paramedian pararectal incision was performed and then photographed (Figure 3). This incision was larger than the primary. The bovine pericardium used is a Brazilian one (bovine pericardium Hpbio®).The adhesions were assessed and catalogued according to the Adhesion Scoring Group - EUA, 1994 designated MCASM (more comprehensive adhesion score method). Though progress has been achieved, it is difficult to point out the best method to identify and quantify aspects of focal adhesion. The new method establishes more efficient identification of the place adhesion is formed and also the identification of the adhesion severity. The adhesion fixation grade was classified from 0 to 3 and the adhesion extension grade from 0 to 4. These grades can be summed or multiplied independently. The grades in the present analysis were summed. The abdominal wall suture results were used as control (internal control) because only half of the suture was covered by the bovine pericardium. In the uterus, the inside control was the posterior uterine wall and external control was characterized by the comparison of CG and EG. The other classification utilized was ¨Adhesion Extension in Experimental Lesion¨(AEEL).

Figure 3. Midline lesion (MLL). External paramedian pararectal laparotomy showing adhesions covering the entire suture, omentum and the thin bowel fixation.
The analyzed data were: 1 - a number that characterized each animal; 2 - the measure of the incision extension; 3 - the measure of the adhesion extension; 4 - adhesion intensity; 5 - structures related to the adhesion (if the omentum were adhered to the bladder, and the bladder were adhered to the uterus lesion, the sum of the grades would be done separately, according to MCASM). 6 - percentage of the adhesion area related to the lesion extension or related to the membrane; 7 - animal weight; 8 - surgery time in minutes ; 9 - the date the animal was sacrificed; 10 - complications; 11 - reasons for animal exclusion; 12 - Intravenous Cefazolin dosage in the beginning of the surgery; 13 - MCASM-SUM; 14 - MCASM average/ animal; 15 - AEEL-SUM(25); 16 - AEEL average/animal (these two last criteria are from our group research in 1991 in which only the percentage of compromised lesion was used). The same analysis was performed for the uterus lesion. The force-inducing adhesion was catalogued in the following degrees: Degree I - the adhesion inducing lesion showed an average sum less than or equal to 25% of the possible grade for that lesion. Second Degree - the adhesion inducing lesion showed an average sum between 26% and 50% of the possible grade for that lesion. Third Degree - the adhesion inducing lesion showed an average sum between 51% and 75% of the possible grade for that lesion. Fourth Degree - the adhesion inducing lesion showed an average sum higher than 75% of the possible grade for that lesion.
The animal exclusion criteria for the experimental group were: aanimals that did not survive at least three days after the surgery. banimals that developed severe post-operative infection at the place where the surgery took place. canimals that developed intense suture dehiscence after the surgery, with or without infection.
Experimental group exclusion criteria: the experimental group should be excluded if there was animal loss in a rate equal or larger than 60%. Statistical analysis were performed by the Epi Info program. The analyses were based on average weight, surgery time and adhesion grades. AnOVA test and Kruskal Wallis tests were used to assess the data.
The rejection level of the null hypothesis was established in 5% (p<0,05), identified on the table or chart by an asterisk.
RESULTS
Two animals were excluded from the Control Group (CG) and one from the Experimental Group (EG). Animal 1 was excluded because of its death on the first day after the surgery and animals 2 and 3 because of severe infection. Consequently the study was concluded with eight animals in the CG and nine animals in the EG.The average weight of the animals were in 12.50 Kilograms in the CG and 15.66 Kilograms in the EG (p=0.5952). The average time of the surgery was 78.25 minutes in the CG and 77.89 in the EG (p=0.9609). The structures involved in the adhesion were related either to the abdominal wall or to the uterus. They were the omentum, the bladder and the bowel (mainly the thin one) with higher adhesion scores.
Through MCASM for the second lesion (Figure 4) were observed an average of 4.62 in the CG versus 7.55 in the EG (p=0.0055).

Figure 4. Midline lesion: average score for both groups (CG and EG) according the classification used. MCASM-M = average score of the group. AEEL-M = average score of the group. CG= control group. EG= experimental group.
Using the AEEL was observed an average of 2.75 in the CG versus 4.77 in the EG (p=0.0155). For the uterine lesion (Figure 5), through MCASM the results were an average of 6.50 in the CG and 6.00 in the EG (p=0.7188) and the AEEL , the results were an average of 4.87 in the CG and 4.33 in the EG (p=0.6155).
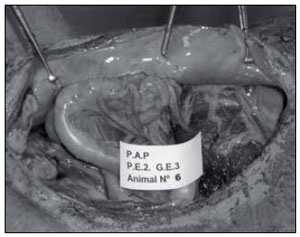
Figure 5. Uterine lesion: average score for the groups (CG and EG) according to the classification used.
DISCUSSION
The abdominopelvic adhesions have been object of a lot of studies over the past years, not only because of the suffering that they cause in patients but also because of the costs for the health care systems. These consequences are well evidenced by bowel occlusion or sub-occlusion, infertility and chronic pelvic pain (Oelsner et al., 1994; Lower et al., 2004; Parker et al., 2004).
As noted in the introduction of this paper, barrier methods, including membranes, gels, viscous solutions or not, have dominated the research in this area. Although researchers have not found the ideal substance yet, there is no doubt that some of these methods are useful in clinical practice. Some authors (Johns, 2001; Ahmad et al., 2008) found pelvic adhesion prevention level 1 in three barrier methods (Interceed®, Seprafilm®, GoreTex®).
In our country, there is no tradition of research in this field, except for rare cases (Beck et al., 2000). Another factor that complicates investigation of barrier methods is the cost of certain membranes. Regardless, one cannot suggest the use of a specific method of adhesion prevention, as research in recent years offers no degree of security. The proposal for studying the pericardium can be attributed to two aspects: first, the apparent similarity to the Gore-Tex, and second, the fact that the pericardium is routinely used in cardiac surgery in Brazil, with relatively low cost (Braile et al., 1998).
The role of the effectiveness of lesion-inducing peritoneal adhesions, as emphasized by several authors (Florencio et al., 1991; diZerega, 1997; Mutsaers, 2002), has been well documented in this paper, in which adhesions occurred in an intense and extensive form. The choice of inducing lesion, can lead to two types of errors: 1-a small inducing lesion force, can overvalue a method of prevention and 2-with an excessive lesion inducing force, can assess ineffectively a method that could be effective in humans, in daily practice. In this study we choose strong inducing lesions (adhesions in more than 90% of dogs), independently of the location the majority of adhesions showed a high score on the day of observation (the sixth day after surgery), which allowed this research to be catalogued within the criteria stipulated in the material and methods, such as inductive study with grade IV lesion. Some authors (Hurst, 1999; Rodgers et al., 1998) used in their research, such lesions without binding force, and they reached excellent results in animals but those results were not subsequently confirmed in humans. In this experiment, some dogs had a score two times greater than the maximum value, also evident in the GE second lesion, in which six of the nine dogs had two structures attached to the lesion site. For example: the dogs that developed omentum adhesion, bowel and omentum adhesion, bladder and bowel adhesion, with a maximum adhesion area, would achieve a score three times greater than the maximum specified. The internal control of the uterus, the posterior uterine wall in such case, showed no adhesion, while the second lesion had high levels of adhesion, mainly in the part that was not used protection in the suture. This fact points out the importance of ischemic injury in the genesis of adhesions.
Once adhesions developed in 100% of the first lesion and in 90% of the second lesion it is possible to claim that the high-strength adhesion of peritoneal sutures are potentially ischemic. nagele et al., 1996 and Sharma et al., 2002 observed a rate of 10% to 30% of adhesions in non-ischemic conventional sutures in the peritoneum and lower rates in the absence of sutures. In this experiment, the second lesion reached significant levels showing that the BP acted inducing adhesion (Figure 4). However, the examination of adhesion rates in the uterus lesions did not show any difference between CG and EG (Figure 5).According to the results we must emphasize the importance of the classification chosen for this research to be carried out. If we had chosen a simple classification that takes into account only the injured area and not the structures involved and attached to the lesion, as was the case of the classification used in previous studies (Florencio et al., 1991; Rodgers et al., 1998), the results could be totally different and probably would not show that the bovine pericardium caused more adhesions instead of preventing them in the second lesion. Some considerations should be made about the pericardium regarding to its preservation and preparation in order to be used in humans. The product is conserved in a formaldehyde solution and it is valid up to four years. In this experiment, we removed the formaldehyde in five saline washes though only two to four washes are normally necessary. Handling of bovine pericardium is easy and non-absorbable suture does not break the membrane. Up to the present we are not able to assess the impact of the pericardium preservative on the abdominal cavity.
8. diZerega GS. Biochemical events in peritoneal tissue repair. Eur J Surg. 1997; S577:10-16.