JBRA Assist. Reprod. 2012;16(06):329-331
ARTIGO ORIGINAL
doi: 10.5935/1518-0557.2012.16.6.03
Elective embryo transfer
1Clínica Monteblanco, Chile
2Unit of Reproductive Medicine Clínica las Condes, Chile
3Program of Ethics and Public Policies in Human Reproduction, University Diego Portales, Chile
ABSTRACT
Multiple birth, due the transfer of more than one embryo, constitutes the most serious complication for both mother and children after assisted reproductive technology. Embryo cryopreservation allows the sequential transfer of the whole cohort of embryos generated in one ART cycle, either by electively transferring one embryo (eSET) or two embryos (eDET). We reviewed the database of ART procedures reported to the Latin American network of ART (REDLARA) by 140 institutions in 2010. We identify eSET, eDET, and 3ET and 4ET when three and four or more embryos were transferred, respectively, and none was cryopreserved. We analysed the outcome of 808 eSET, 5,978 eDET, 4,398 3ET and 968 4ET. Women that underwent eSET and 4ET were older than women that underwent eDET and 3ET (p<0.0001). The mean number of oocytes recovered was higher in women undergoing eDET (12.3) than in women undergoing eSET (6.7); 3ET (9.0); and 4ET (9.8) (p<0.0001). The clinical pregnancy rate reached 18% with eSET; 43% with eDET; 34% with 3ET; and 35% with 4ET. the proportion of twin delivery was 0.9% with eSET; when more than one embryo were transferred, the twin rate did not differ significantly: 22% with eDET; 21% with 3ET and 23% with 4ET. However, high order multiple births (≥3newborns) increased significantly with both 3ET (3.0%) and 4ET (4.4%). that neither the weight nor gestational age at delivery of singletons were associated to the number of embryos transferred. With the proper counselling regarding cumulative pregnancy rate and risks associated with twin pregnancy, and a fixed payment for all ET performed, we expect more couples -and physicianswould undergo eSET.
INTRODUCTION
Multiple birth constitute the most serious complication for both mother and children after Assisted Reproductive Technology (ART). For the mother, multiple pregnancies are associated with higher risks of hypertensive disorders, anaemia and haemorrhage during pregnancy 1;2. For the foetuses, multiple pregnancy increases significantly the risk of preterm birth and perinatal morbidity and mortality3.
Since our ability to predict the capacity of the embryo to implant is limited, the transfer of more than one embryo increases the possibility of transferring one normal embryo, and thus obtaining a pregnancy. It is for this reason that clinicians, many times, influenced by couples, transfer more than one embryo, hoping to maximise the outcome of a single cycle. Couples in countries with little or no reimbursement for infertility-related procedures are even more prone to such attitude 4.
Embryo cryopreservation allows the sequential transfer of the whole cohort of embryos generated in one ART cycle, either by electively transferring one embryo (eSET) or two embryos (eDET). Elective SET has been shown to be an effective strategy to minimise the risk of twins without compromising IVF cumulative success rates5, while eDET have shown to maintain a higher pregnancy rate by exposing women to high twin-pregnancy rates 6-8.
The objective of this study is to compare the outcome of elective single embryo transfer (eSET); elective dual embryo transfer (eDET); three-embryo transfer (3ET); and four-and-more embryo transfer (4ET).
MATERIALS AND METHODS
We reviewed the database of ART procedures reported to the Latin American network of ART (REDLARA) by 140 institutions in 2010. We identify eSET and eDET, when one or two embryos were transferred, and the rest of the cohort of embryos were cryopreserved; an 3ET and 4ET when three and four or more embryos were transferred, respectively, and none was cryopreserved. The data analysed included age of the female partner, number of oocytes recovered, number of embryos transferred, stage of development at embryo transfer (ET), and clinical outcome. Clinical outcome was defined as clinical pregnancy rate per ET (CPR/ET), abortion rate, newborn weight in grams, and gestational age in completed weeks at the time of delivery. Precise definitions can be found in the ICMART glossary (ref).
STATISTICAL ANALYSIS
Categorical variables were compared with Fisher´s exact test. Interval variables were compared either with Student´s t-test or one-way AnOVA, depending on the number of strata of the categorical variable. Multiple variable analysis was performed either with lineal regression or logistic regression, depending on the nature of the outcome variable. We considered a p-value les than 0.05 to be statistical significant.
RESULTS
We analysed the outcome of 808 eSET, 5,978 eDET, 4,398 3ET and 968 4ET. Table 1 shows the demographic data of these ET. Women that underwent eSET and 4ET were older than women that underwent eDET and 3ET (p<0.0001). The mean number of oocytes recovered was higher in women undergoing eDET (12.3) than in women undergoing eSET (6.7); 3ET (9.0); and 4ET (9.8) (p<0.0001). Also, the mean number of embryos cryopreserved was higher in cases of eSET (4.4) than in eDET (4.0) (p=0.0468)- The majority of embryos were cryopreserved at cleaving stage, both in eSET (56%) and eDET (63%).
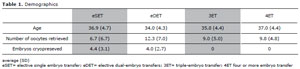
Table 1. Demographics
In both, eSET and eDET, only 14% of ET were performed at blastocyst-stage, while 2% of 3ET and 4ET were performed at blastocyst-stage. Table 2 shows the outcome of ET. The miscarriage rate was the highest when eSET was performed (21%), and the lowest when eDET was performed (14%). However, after correcting for age, we found that the number of embryos transferred was not associated to the odds of miscarriage. The CPR/ET reached 43% when eDET was performed. When more than two embryos were transferred, the CPR reached 34% (3ET) and 35% (4ET). The CPR/ET was significantly lower when eSET was performed (18%). nevertheless, in women aged less than 35 years, the CPR/ET when eSET was performed reached 30%. Multiple variable logistic regression showed, that after correcting for the age of woman and embryonic developmental stage, the OR for CPR/ET was significantly higher only when eDET was performed (OR 3.0, 95% 2.5-3.6). Table 3 shows perinatal outcome. As expected, the proportion of twin delivery was the lowest when eSET was performed (0.9%). When more than one embryo were transferred, the twin rate did not differ significantly. Twin delivery reached 22% when eDET was performed, 21% when 3ET and 23% when 4ET was performed. However, high order multiple births (≥3newborns) increased significantly with both 3ET (3.0%) and 4ET (4.4%). We analysed the perinatal outcome as expressed by the mean weight and mean gestational age at birth of singletons and compared them, after eSET, eDET, 3ET and ≥4ET. We did not find any significant difference neither in the weight (p=0.118) nor in the gestational age at delivery (p=0.336). Multiple variable lineal regression, after correcting for woman´s age and gestational age at delivery, demonstrated that neither the weight nor gestational age at delivery of singletons were associated to the number of embryos transferred.
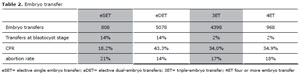
Table 2. Embryo transfer
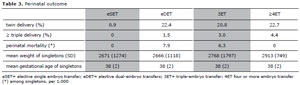
Table 3. Perinatal outcome
DISCUSSION
A multiple pregnancy is a clinical risk to both infant and mother following IVF treatment. Children born after IVF had a poorer obstetric outcome compared with children from the general population. Singletons, when analysed as one group, irrespective of whether the children were born after eSET, non-eSET or DET, also had a poorer obstetric outcome with higher rates of preterm and LBW compared with singletons in the general population 9.
We found that eSET was significantly associated with a lower frequency of multiple delivery and abortion rate. We were not able to prove a difference in perinatal outcome of singletons, expressed as the mean weight and gestational age at delivery.
It is interesting that the transfer of ≥2 embryos yielded similar twin-delivery rate, around 20%, among eDET, TET and FET. However, the transfer of ≥3 embryos was significantly associated with an increase in the proportion of triple-deliveries.
Thus, the only way to reduce the risk of multiple gestation and delivery is to enforce eSET. Since eSET is significantly associated with a reduction in the CPR, many clinicians and patients might be reluctant to undergo eSET and might prefer to undergo at least eDET. At least, this have been the experience in different countries. Per example, Murray et al found that maintaining existing rates of pregnancy and offering a fixed charge for all embryo transfers resulting from an oocyte recovery may encourage more couples to consider eSET10.
In general, patients’ preferences for a singleton or twins are not definitive during IVF treatment. Possible explanations of a shift in preference are that pregnant patients attuned their preferences to what they expect their pregnancy to result in, whereas non-pregnant patients shifted towards a preference for twins in order to be able to fulfil their ultimate child wish11. Furthermore, when exposed to the risks of multiple births and the option of selecting elective single-embryo transfer, the use of complex persuasive communication techniques on a student population to promote eSET preferences is more successful at promoting eSET than merely reporting educational content 12.
On the other hand, physicians are reluctant to perform eSET. In a study published by Van Peperstraten a total of 107 professionals participated. The most frequently mentioned barriers to eSET use were suboptimal success rates associated with cryopreservation (96%) and not seeing twin pregnancies as a complication (79%) 13.
We found that patients undergoing eSET cryopreserved in average 4 embryos, thus they have four further intents of eSET. Thus, the outcome that should be discussed with the patient is the cumulative CPR, rather than the CPR after a fresh transfer. Probably, a main barrier to do this is the oeconomical, since in Latin America most of the couples must pay for the treatments by themselves, with little or no governmental support.
The present study has the strength that corresponds to the analysis of a robust database. The RLA keeps the data of ca. of 80% of ART procedures performed in Latin America since 1990. The clinics are used and trained in providing such data, and the data is periodically verified by an independent committee. However, an important weakness of this study is that it corresponds to an observational study. As such, the intervention i.e. the number of embryos transferred were not randomised, and no causality can be inferred. Furthermore, some unmeasured variables such as the experience of the clinician or laboratory, may influence the outcome of the procedure.
With the proper counselling regarding cumulative pregnancy rate and risks associated with twin pregnancy, and a fixed payment for all ET performed, more couples -and physicianswould undergo eSET.