JBRA Assist. Reprod. 2012;16(06):332-336
ARTIGO ORIGINAL
doi: 10.5935/1518-0557.2012.16.6.04
Trends in the number of transferred embryos, clinical pregnancy rate and multiple pregnancy rate in Latin America: 1998 through 2008
1Clínica Monteblanco, Chile
2Unit of Reproductive Medicine Clínica las Condes, Chile
3Program of Ethics and Public Policies in Human Reproduction, University Diego Portales, Chile
ABSTRACT
Background. Reducing the rate in IVF of multiple births and associated perinatal complications has become the major challenge in Latin America, due to is association with a significant increase in the prematurity, and perinatal mortality.
methods. We selected all procedures involving the transfer of IVF embryos, reported to the Latin America Registry of ART, initiated between January 1998 and December 2008. A Poisson regression analysis was performed, stratified by woman´s age to analyse the trend in the transfer of 2, 3 and ≥4-embryos and ≥triple-pregnancy rate.
Results. A total of 164,874 IVF/ICSI transfers were considered. Overall, there was a decline in the proportion of procedures performed in women aged ≤34 years old from 51% to 43%; and an increase of ICSI procedures from 61% to 86%. All age groups experienced a reduction in the proportion of ≥4-embryos transfers and an increase in that of 2-embryo transfers. Overall, the clinical pregnancy rate improved from 29% to 35% (p=0.01); and the incidence of ≥triple-pregnancy decreased from 8% to 3% in 2008 (p<0.001), while twin pregnancy remained stable (~20%)
Conclusions. Our data support the policy of transferring less embryos. It shows a decline in the mean number of embryos transferred and proportion ≥ 4-embryos transfers. Moreover, it reports a clinical pregnancy rate which instead of being reduced, has shown an increase over the 10-year period.
INTRODUCTION
The first IVF-baby in Latin America was born in Colombia in 1984. This technology spread rapidly all over Latin America generating a substantial increase in the number of patients gaining access to Assisted Reproductive Technologies (ART). The current need for ART procedures, however, is by far underserved, and great disparity persists in the access to such technology1.
The latest report by the International Committee Monitoring Assisted Reproductive Technology presents worldwide information about ART procedures performed in 20032. At that time, the number of cycles reported by Latin-American centers represented only 2.3% of the 932,415 cycles performed worldwide. Expressed as the ratio of ART cycles per million inhabitants, the disparity in access to ART is even more striking: countries like Sweden, Denmark and Belgium perform between 1,000 to 2,000 cycles per million inhabitants, whilst countries in Latin America perform between 33 and 109 cycles per million inhabitants2. In countries where ART is reimbursed or covered by public health insurance, the mean number of embryos transferred is much smaller than the number of embryos transferred in countries where ART is funded by each couple3.
Current economic policies in Latin America cause that only a small percentage of the gross domestic product is allocated to health related expenditures. Furthermore, the majority is diverted to private health expenditure such as insurance companies, who do not cover infertility-related procedures4. Thus couples have to rely on their own resources to fund their treatments which limits the number of infertile couples with access to treatment and the number of opportunities that couples have to receive ART treatments.
In order to achieve successful outcomes while minimising the number of ART procedures attempts, multiple embryos are transferred into the uterus which in term increases the chances of pregnancy5. However, this strategy also increases in the rate of twin and high order multiple pregnancies6.
At a regional level, Latin America shows comparable clinical outcomes to those of developed countries. Similar clinical pregnancy rates and delivery rates, are reported, although with a larger number of embryos transferred, and regardless of the age of the female partner2.
Reducing the number of embryos transferred with a reduction in the rate of multiple births and associated perinatal complications has become the major challenge in Latin America, since multiple pregnancies are associated with a significant increase in the prematurity, and perinatal mortality1. Furthermore, the increase in family disorders mainly absorbed by women, and high individual and insurance costs to cover neonatal expenses are also issues that need to be addressed. This study examines trends in embryo transfer practices and clinical and multiple pregnancy rates for assisted reproductive technologies performed in Latin America between 1998 and 2008. Given the strong association between number of embryos transferred and multiple birth risk7,8, assessment of embryo transfer practices is essential to understanding the multiple gestation and birth risk associated with assisted reproduction. Our aim is to document the decline in the number of embryos transferred, and the impact such shift might have had on clinical pregnancy and multiple gestation rates.
MATERIAL AND METHODS
Study population
The Latin American Registry of Assisted Reproductive Technologies (RLA) was established in 1990 as the first multinational registry in the world. Today, it registers more than 80% of the cycles performed in the region, including countries such as Mexico in the north and Argentina/Chile in the South.It corresponds to a registry of summary cases, in which every year each centre voluntarily summarises the characteristics and outcomes of the cycles performed, and uploads said information in a web page maintained by RLA. The administrative office in Santiago, Chile, periodically recovers and analyses this data for consistency. Once all the information is cleared, and the centre is checked as accredited by the RED, the data is included and published by the RLA as part of yearly report, available on the web.For analysis we selected all procedures involving the transcervical transfer of IVF embryos (either through ICSI or standard IVF) into the uterus, with the woman’s own eggs, initiated between January 1998 and December 2008. A total of 164,874 IVF/ICSI transfers were considered.We focus in the proportion of embryo transfers in which 1, 2, 3 and ≥4 embryos were transferred. The transfer of 5 and 6 embryos represented a minor proportion, thus we preferred to categorised them under the transfer of ≥4 embryos.
Data analysis
The number of embryo transfers in IVF/ICSI cycles, in which 1, 2, 3, and ≥4 embryos were transferred; the number of clinical pregnancies; and the number of multiple pregnancies were analysed. Clinical pregnancy was defined as the identification of at least one gestational sac by ultrasound, whereas multiple pregnancy was defined as the identification of one or more gestational sac(s)9.The annual proportion of transfers with 1, 2, 3 and ≥4 embryos embryos transferred, and clinical pregnancy rate and multiple pregnancy rate were investigated stratified by woman’s age category: ≤34 years old, between 35 and 39 years old, and ≥40 years old.
Statistical analysis
We performed a Poisson regression analysis, stratified by woman´s age to analyse the trend in the transfer of 2, 3 and ≥4-embryos and ≥triple-pregnancy rate, using Stata Software package, version 11,0 (Texas, USA).
RESULTS
Embryo transfers
Table 1 shows the number of IVF/ICSI embryo transfers performed between 1998 through 2008, according to the woman’s age category and type of fertilisation. Overall, there was a two-fold increase in the number of procedures registered; a decline in the proportion of procedures performed in women aged ≤34 years old from 51% to 43%; and an increase of ICSI procedures from 61% to 86%
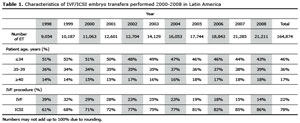
Table 1. Characteristics of IVF/ICSI embryo transfers performed 2000-2008 in Latin America
Number of embryos transferred
Figure 1 shows the decline in the mean number of embryos transferred between 1998 and 2008. The mean number decline from 3.3 in 1998 to 2.5 2008, which was statically significant (p<0.001). Table 2 shows the distribution of IVF/ICSI embryo transfers according to the number of embryos transferred in each age category. All age groups experienced a reduction in the frequency of ≥4-embryos transfers, and an increase in the proportion of 2-embryo transfers.
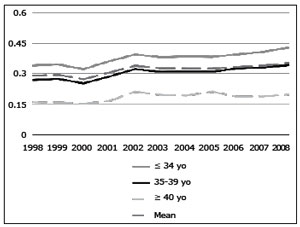
Figure 1. Clinical pregnancy rate per embryo transfer in women undergoing IVF/ICSI cycles according to woman’s age category RLA 1998-2008
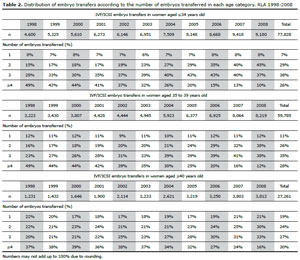
Table 2. Distribution of embryo transfers according to the number of embryos transferred in each age category. RLA 1998-2008
Women aged ≤34 years old experienced an increase in the proportion of 2-embryo transfers from 15% in 1998 to 45% in 2008 (p<0.001) and a decrease in the proportion of ≥4-embryo transfers from 49% to 10% (p=0.006). Similar findings were reported by women aged 35 to 39 years with an increase in the proportion of 2-embryo transfers from 16% to 38% (p=0.001) and a decline in the proportion of ≥4-embryo transfer (p<0.001). This trend was less pronounced in women aged ≥40 years experienced the proportion of 2-embryo transfers increased from 22% to 30% (p=0.075) and the proportion of ≥4-embryo transfers decreased from 37% to 16% (p=0.01).
Clinical Pregnancy
Figure 1 shows the clinical pregnancy rate per embryo transfer in each age category between 1998 and 2008. Overall, the clinical pregnancy rate improved from 29% in 1998 to 35% in 2008 (p=0.01). In women aged ≤34 years this improvement was from 34% to 43% (p<0.001); in women aged 35 to 39 years it was from 27% to 34% (p<0.001); and in women aged ≥40 years it was from 16% to 20% (p=0.047).
Multiple Pregnancy
Figure 2 shows the distribution of clinical pregnancies according to gestational order in women who underwent IVF/ICSI between 1998-2008. Overall, the incidence of ≥triple-pregnancy decreased from 8% in 1998 to 3% in 2008 (p<0.001), while the proportion of twin pregnancy remained stable (~20%).
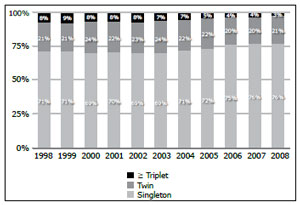
Figure 2. Clinical pregnancies according to gestational order in women undergoing IVF/ICSI. RLA 1998-2008
Table 3 shows the distribution of clinical pregnancies according to gestational order in each woman’s age category. The frequency of ≥triple pregnancy, from 1998 to 2008, decreased , from 10% to 5% (p<0.001) in women aged ≤34 years; from 6% to 3% (p<0.001) in women aged 35 through 39 years and 4% to 2% (p=0.058) in women aged ≥40 years.
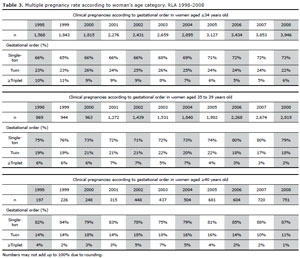
Table 3. Multiple pregnancy rate according to woman’s age category. RLA 1998-2008
Table 4 shows the incidence risk ratio for ≥ triple pregnancy adjusted for woman´s age category, stratified by quartile of the mean number of transferred embryos. As seen, the incidence risk ratio for ≥triple pregnancy diminished significantly over time in the groups where less embryos were transferred. In the two groups where more embryos were transferred, the decrease in the incidence risk ratio did not change significantly over time.
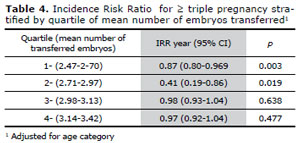
Table 4. Incidence Risk Ratio for ≥ triple pregnancy stratified by quartile of mean number of embryos transferred1
Table 5 shows the perinatal outcome of babies born due to FIV/ICSI performed between 1998 and 2008 according to the gestational order. The risk of perinatal mortality increased significantly with higher gestational orders.
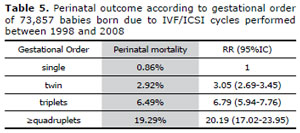
Table 5. Perinatal outcome according to gestational order of 73,857 babies born due to IVF/ICSI cycles performed between 1998 and 2008
DISCUSSION
The number of infertile couple undergoing assisted reproductive technologies increased significantly in the period analysed, as did the clinical pregnancy rate per embryo transfer, regardless of the woman’s age-category. When focusing on the success such procedures, attention should also be given to its complications. The most important being that of multiple pregnancy which is significantly associated with preterm delivery and perinatal morbidity and mortality.
In Latin America, the frequency of ≥triple pregnancy rate has halved in all woman’s age categories over this 10-year period, while the proportion of twin pregnancy remained stable. Multivariate analysis showed that the most important factor that accounted for this decline is the significant decrease in the mean number of embryos transferred. The constant, yet minor, decrease in the mean number of embryos transferred significantly lowered the frequency of ≥triple pregnancy, but showed no significant effect in the proportion of twin pregnancies. The increase seen in the proportion of three-embryo transfers may have countered,the effect caused by the reduction in the proportion of ≥four-embryo transfers.
Importantly, this decline in the number of embryos transferred was not associated with a decline in the clinical pregnancy rate, on the contrary, the clinical pregnancy rate per embryo transfer improved significantly between 1998-2008 in all age categories. This suggests that other unmeasured factors improved over time. One of these might be the transfer of embryos in later stages of development, allowing for a better selection and improved implantation rates.
In an attempt to diminish the ART-related multiple pregnancies epidemic, countries like Sweden, Belgium and Japan have implemented strict policies and support the elective transfer of one embryo, with a clear reduction in the multiple pregnancy rate (10-14). This is feasible in countries where ART procedures are covered by health insurance and thus have some control over ART practice. This is difficult in Latin America, where ART procedures are mainly covered by infertile couples, and the open market economy dictates strong competition between different ART centres, which have the tendency to maximise results, regardless of multiple pregnancy rate.
Nevertheless, we found that practice in the region is moving towards the right direction with more work needed for reducing the number of embryos transferred. Our data support the policy of transferring less embryos. It shows a decline in the mean number of embryos transferred and proportion ≥ 4-embryos transfers. Moreover, it reports a clinical pregnancy rate which instead of being reduced, has shown an increase over the 10-year period.