JBRA Assist. Reprod. 2012;16(06):320-328
ARTIGO ORIGINAL
doi: 10.5935/1518-0557.2012.16.6.02
Assisted reproductive technologies in Latin America: The Latin American Registry, 2010
1Unit of Reproductive Medicine Clínica las Condes, Chile
2Program of Ethics and Public Policies in Human Reproduction, University Diego Portales, Chile
3Clínica Monteblanco, Chile
4Fertipraxis-Centro de Reprodução Humana-RJ, Brasil
ABSTRACT
Background: This 21st report represents the results of ART procedures performed during 2010 by 140 centers from 13 countries in Latin America. Furthermore, this is the first time, a multinational registry is performed on a case-by-case bases.
Methods: All centers reported their ART procedures electronically and their data was accepted after consistency checks were performed and the institution, certified by an accreditation team. A total of 37,853 initiated ART cycles included 3,731 IVF cycles; 22,637 ICSI cycles; 5,157 FET and 6,320 OD embryo transfers, plus 8 cases of GIFT, which are not described in this report.
Results: The majority (39%) of ET in IVF/ICSI cycles were performed in women age 35-39 years. The delivery rate (DR) per OPU in ICSI and IVF cycles were 28.8% and 30.9%, respectively. The multiple delivery rates in IVF/ICSI cycles were 23.9% (22.1% twins and 1.8% triples). When ≥ 2 embryos were transferred, neither the CPR nor the proportion of twins increased significantly. However, the proportion of triplet increased significantly when ≥3 embryos were transferred. In OD cycles, twin and triplet deliveries were 25.4% and 2.2%, respectively. In FET cycles, twin and triplet deliveries were 17.6% and 1.5%, respectively. Multiple deliveries were associated with a significant increase in preterm delivery and perinatal mortality. The CPR was 18% with eSET and 43% with eDET. In women aged ≤34 years, CPR with eSET was 30% and 52% with eDET. In OD cycles, the CPR with eSET was 29%, and 52% with eDET.
Conclusions: Overall, delivery rates are comparable to most developed countries in the world. However, REDLARA has to enforce the reduction in the number of embryos transferred in IVF/ICSI and OD cycles, in order to prevent multiple births and decrease the corresponding perinatal complications.
RESUMO
Objetivo: Este 21º relato representa os resultados de procedimentos de RA realizados em 2010 por 140 centros de 13 países na América Latina. Pela primeira vez, um registro multinacional é realizado caso-a-caso.
Métodos: Todos os centros registraram seus procedimentos eletronicamente e os dados foram aceitos após checagem de consistência, cada instituição certificada por acreditadores. Do total de 37,853 ciclos iniciados de RA , foram 3,731 ciclos de FIV, 22,637de ICSI, 5,157 transferências de embriões congelados e 6,320 transferências em ciclos de Ovo-Doação(OD), além de 8 casos de GIFT.
Resultados: A maioria (39%) das TE nos ciclos de FIV/ ICSI foram realizadas em mulheres de 35-39 anos. A taxa de partos por aspiração (OPU) nos ciclos de ICSI e FIV foi de 28.8% e 30.9%, respectivamente. Os nascimentos múltiplos em FIV/ICSI foram de 23.9% (22.1% duplos e 1.8% triplos). Quando transferidos ≥ 2 embriões, nem a taxa de gestação clínica (CPR) ou a proporção de duplos aumentou significativamente. Todavia, a proporção de triplos aumentou significativamente quando ≥3 embriões transferidos. nos ciclos de OD, nascimentos duplos e triplos foram 25.4% e 2.2%, respectivamente. nas transferências de embriões congelados (FET), relatos de duplos e triplos foram 17.6% e 1.5%. Partos múltiplos foram associados a aumento significativo de nascimentos pré-termo e mortalidade perinatal. A taxa de gravidez clínica foi de 18% com a transferência seletiva de 01 embrião (eSET) e 43% na dupla (eDET). nas mulheres ≤34 anos, a CPR com eSET foi 30% e 52% com eDET. nos ciclos de OD, estas taxas de gravidez clínica foram de 29% com e-SET , e 52% com eDET.
Conclusões: Em geral, as taxas de nascimentos são comparáveis aos países mais desenvolvidos. Todavia, a REDE deve reforçar a necessidade de transferir menor número de embriões nos ciclos de RA, a fim de prevenir nascimentos múltiplos e diminuir as consequentes complicações perinatais.
INTRODUCTION
This report corresponds to the twenty first edition of the Latin American Registry of Assisted Reproductive Technology (RLA). Reports from 1990 through 1998 are available as printed copies; from 1999 through 2009 are available as PDF files to be downloaded from the web page of Red Latino Americana de Reproducción Asistida (REDLARA) at www.redlara.com.
The main objectives of RLA include: to register the number and characteristics of assisted reproductive techniques (ART) procedures performed in Latin America (LA); to register their outcomes, including controlled ovarian hyperstimulation, pregnancies and perinatal outcomes; to register the complications associated with ART procedures and the frequency and characteristics of congenital malformations; and to evaluate trends in multiple pregnancy and delivery, preterm birth, perinatal mortality and others.
MATERIAL AND METHODS
Data collection:One hundred and forty centers from thirteen countries reported data involving ART procedures performed from January to December 2010. ART procedures included in vitro fertilization (IVF), intracytoplasmic sperm injection (ICSI), gamete intrafallopian transfer and similar techniques (GIFT), oocyte donation (OD), frozen/thawed embryo transfer (FET), prenatal genetic diagnosis and screening (PGD), and assisted hatching (AH). The main methodological characteristic of the current report is that for the first time the data of each treatment cycle was recorded independently, instead of a summary of cases, as it was reported until now, thus, this is the first multinational case by case registry. This way of collecting data has two main advantages. First, it reduced the work of those responsible for reporting data from each center, and second, a case-by-case multinational register, allows for more sophisticated biostatistics and epidemiological analysis. As in the past, each center provided their data on voluntary bases. Furthermore, before the data is accepted, each center has to undergo periodical accreditation visits, where a clinician and an embryologist from a different country, evaluate the professionals, the infrastructure and equipment of the center, together with their quality control programs and their consent forms. Furthermore, the data provided by the center to the RLA is carefully and thoroughly analyzed. Each center has an individual password in order to access the RLA-server, where the center can upload the data of each cycle. The data can be uploaded either by filling a specially designed page each time a new case is performed, or by uploading an Excel file whenever possible. The central office of RLA gains immediately access to the data, and checks for inconsistencies and resolve any further question with the center.
Data validation: The data provided by each centers is checked for inconsistency by the program; and any error is discussed with the center, and the data is rectified if necessary. The truthfulness of the data reported by each institution is checked as part of the periodic accreditation process conducted by a biologist and a clinician from different countries.
Limitations of data collection: Some centers do not have complete follow-up of each pregnancy. This is especially so in institutions not associated with obstetric units. Our calculations are that missing data is in the order of 5% of pregnancies. From a different perspective, not all centers performing ART belong to REDLARA. We estimate that the RLA registers more than 80% of ART procedures performed in Latin America.
Statistical analysis: Chi square test was used to analyze independence of categorical variables. When multiple variable analyses were performed, i.e. logistic regression or lineal regression, the dependent variables were considered significant if the confidence interval of the odd ratio (OR), or regression coefficient did not cross the non-significant value. A p-value <0.05 was considered as statistically significant. When comparing two outcomes, the risk ratio (RR), and its corresponding 95% confidence interval (95%CI) are presented.
RESULTS
Participating centers: One hundred and forty (140) centers belonging to 13 countries reported their ART procedures performed during 2010 (Annex I). These represent five more centers than those reporting in 2009. The new institutions belong to Argentina, Brazil, Ecuador and Mexico.
Size of participating institutions:The number of initiated cycles corresponds to the sum of initiated cycles of IVF/ICSI/ GIFT, and embryo transfers, both FET and OD. The average number of initiated cycles registered by the clinics was 268. More than half of the centers registered less than 150 cycles, whereas only three centers registered more than one thousand cycles. The distribution of the clinics according to the number of cycles registered is as follows: 27%, ≤ 100 cycles; 36% between 100 and 250 cycles; 24% between 251 and 500 cycles; 11% between 500 and 1,000 cycles; and only 2%, ≥ 1,000 cycles.
ART procedure and access:The total number of ART procedures registered by the RLA was 37,853. Of these, 47% (n=17,673) were reported by Brazil; 22% (n=8,336) by Argentina; and 12% (n=4,433) by Mexico (table 1). Out of 26,3736 initiated autologous-cycles, 3,731 (14%) corresponded to IVF, and 22,637 (86%) to ICSI cycles. One hundred and twenty six clinics registered 5,157 FET cycles. And one 127 clinics reported 6,320 OD cycles. In 56% of TABELA these cycles, the eggs were donated from pure donors, i.e. women that underwent controlled ovarian hyperstimulation (COS) and oocyte pick up with the only purpose of donating their oocytes; and 44% were egg-sharing, i.e. patients undergoing COS and oocyte pick-up, for an autologous treatment and simultaneously donated a proportion of their gametes. Table 1 also shows access to ART procedures in LA, expressed as the total number of initiated cycles per million women aged 15 to 45 years.
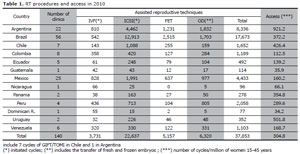
Table 1. RT procedures and access in 2010
Pregnancies and deliveries: Tables 2a and 2b show the clinical pregnancy rate (CPR) and delivery rate (DR) of ART procedures performed in 2010. In the case of ICSI cycles, the overall CPR and DR per oocyte pick-up were 28.8% and 22.1%, respectively. These rates were marginally better in the case of IVF cycles: 30.97% and 25.63%, respectively (table 2a).
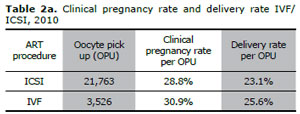
Table 2a. Clinical pregnancy rate and delivery rate IVF/ ICSI, 2010
In both instances, the difference reached statistical significance, however the lack of random distribution of subject in each treatment category, does not allow for conclusions to be obtained. The RR for clinical pregnancy per OPU was 1.07 (95% CI 1.01-1.13); and for delivery rate per OPU was 1.10 (95% CI 1.03-1-17). In OD cycles, the clinical pregnancy rate and delivery rate were 47.0% and 38.6%, respectively. In FET cycles, the clinical pregnancy rate and delivery rate were 29.3% and 22.5%, respectively. These rates were higher in FET with OD: 32.4% and 24.7%, respectively (table 2b).
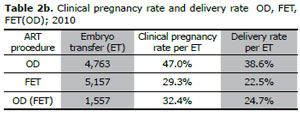
Table 2b. Clinical pregnancy rate and delivery rate OD, FET, FET(OD); 2010
Age of women undergoing ART procedures:The mean age of women undergoing IVF/ICSI/GIFT was 36 years (SD 4.7). Figure 1 shows the age distribution of women undergoing IVF/ICSI/GIFT. 37% of initiated cycles were in women aged ≤34 years; 39% in women aged 35 through 39 years; 16% in women aged 40 through 42 years; and 7% in women aged ≥43 years. This accounts for 23% of women ≥ 40 years.
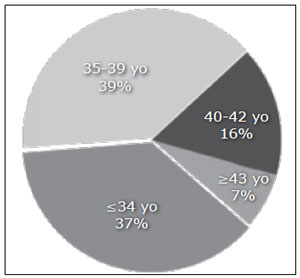
Figure 1. Age distribution of women undergoing IVF/ICSI, 2010
As expected, the delivery rate per embryo transfer was significantly influenced by the age of the female partner. We analyzed DR/ET in the following age categories: women aged ≤34 years; women aged 35 through 39 years; women aged 40 through 42 years; and women aged ≥43 years. DR decreased in all age groups, from 35.5% in the younger women to 8.5% in the oldest group (p<0.001). The eldest women that deliver a baby with autologous oocytes was 49 years at the time of the procedure (Fig. 2a and 2b).
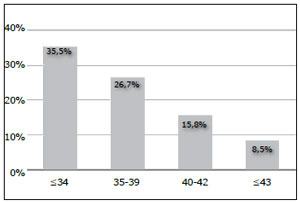
Figure 2. Delivery rate per embryo transfer in different age categories of women undergoing IVF/ICSI, 2010
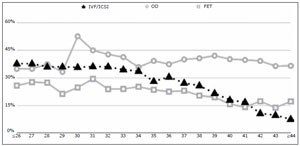
Figure 2b. Delivery rate per embryo transfer according to age of woman, 2010
In cases of OD, DR/ET in oocyte recipients aged ≤34 years (n=523 ET) was 40.2%. In women aged 35 through 42 (n=2,155 ET), was 40.0%; and 37.1% (ET=2672), in women ≥43 years. These differences did not reach mathematical significance.
In cases of FET with OD, women aged ≤34 years had a delivery rate per ET of 28.8%; compared with 23.8% in women aged 35 to 39, and 22.4% in women ≥43 years (p=0.321).
NUMBER OF EMBRYOS TRANSFERRED AND MULTIPLE DELIVERIES
Autologous reproduction: Table 3 shows the outcome of 21, 526 IVF/ICSI embryo transfers. The mean number of embryos transferred was 2.4, identical to the previous report. In 45.2% of cases, two embryos were transferred, and the transfer of 3 and ≥4 embryos represented 34.6% and 7.2% respectively. The overall frequency of multiple delivery was 23.9%, of which, 22.1% were twins and 1.8% triplets and higher, compared with 21.5% and 2.1% respectively in 2009.
The risk of twin delivery increased with the transfer of ≥2 embryos. The risk of twin deliveries was 21.8% when two embryos were transferred, and the transfer of three embryos increased the risk to 1.1 (95%CI 1.0-1.3). The transfer of ≥ four embryos also increased the risk to 1.1 (95% CI 0.9-1.3). The risk of triplet-and-higher delivery also increased significantly with the number of embryos transferred. When only one embryo was transferred, there were no triplets or higher order deliveries; when two embryos were transferred the rate of triplets-and-higher delivery was 0.5%; when three embryos were transferred, the rate of triplets-and-higher delivery increased to 3.3%; with a further increase to 3.9% (p<0.001), when ≥ 4 embryos were transferred.
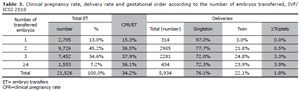
Table 3. Clinical pregnancy rate, delivery rate and gestational order according to the number of embryos transferred, IVF/ ICSI 2010
HETEROLOGOUS REPRODUCTION (OD)
Table 4 shows the outcome of 4,763 OD cycles. The mean number of embryos transferred was 2.4, identical to the previous report. In the majority of cases, two embryos were transferred (58%), and the transfer of ≥3-embryos represented 38% of the cases. The overall frequency of multiple birth was 27.6%; 25.4% were twin delivery, and 2.2% triplets and higher, compared with 23% and 2% respectively in 2009. When compared with the transfer of two embryos, the transfer of three or four embryos increased the relative risk for twins by 1.2 (95%CI 1.00-1.40); and by 1.1 (95%CI 0.8-1.6) respectively. However, the risk of triplet and higher order delivery increased significantly with the transfer of more than two embryos. The rate of triplets increased from nil when one embryo was transferred to 0.5%, 4.8% y 6.8% (p<0.001), when 2, 3 and ≥4 embryos were transferred.
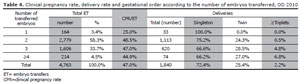
Table 4. Clinical pregnancy rate, delivery rate and gestational order according to the number of embryos transferred, OD 2010
FROZEN/THAWED EMBRYO TRANSFERS(FET)
Table 5 shows 5,157 cases of FET. The mean number of embryos transferred was also 2.4. Two embryos were transferred in 46% of cases. The rate of multiple births was 19.5%; 17.6% were twin delivery (13.1% in 2009); and 1.5% triplets-and-higher delivery (2.7% in 2009). The increase in the rate of multiple-delivery was less profound than in the previous techniques. The rate of triplets-and-higher delivery when one, two, three and ≥four embryos were transferred was 0.0%, 1.3%, 1.9% and 2.3% respectively (p<0.001). Table 6 shows 1,557 cases of FET with donated oocytes. The mean number of embryos transferred was 2.4. Multiple-delivery rate was 23.2%: 21.8% twins and 1.4% triplets. The risk of multiple-pregnancy also increased with the number of transferred embryos, however, this was less accentuated than in the case of fresh transfers (p=0.557).
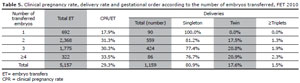
Table 5. Clinical pregnancy rate, delivery rate and gestational order according to the number of embryos transferred, FET 2010
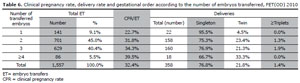
Table 6. Clinical pregnancy rate, delivery rate and gestational order according to the number of embryos transferred, FET(OD) 2010
ELECTIVE SINGE AND DUAL EMBRYO TRANSFER (ESET & EDET)
Elective single embryo transfer (eSET) and elective dual embryo transfer (eDET) accounted for 3.8% (n=810) and 23.6% (n=5,081) respectively, of embryo transfers performed in 2010. This represents an important increase to the previous register, when they represented only 1.0% and 14.2% respectively. The CPR/ET was 18% with eSET and 43% with eDET. Elective SET and DET had higher CPR than non-elective transfers (table 3). The CPR/ET was higher in younger women. In women aged ≤34 years the CPR of eSET and eDET were 30% and 52%, respectively..In OD cycles, the CPR/ET, with eSET was 29% (OR 0.95 95%CI 0.5-1.8), and 52% with eDET (OR 1.2 95%CI 1.0-1.4).
Perinatal outcome: The duration of gestation was reported in 7,126 deliveries (5,281 singletons, 1,704 twins, and 141 ≥triplets). Among singletons, the mean gestational age at delivery was 38 weeks amenorrhea (WA); among twin it was 35 WA; and among ≥triplets it was 32 WA.The risk of preterm birth, (before completing 37 WA), among singletons was 17% (n=898). The relative risk of preterm birth among twin deliveries was 3.9 (95% CI 3.7-4.2), and among triplets-and-higher was 5.7 (95% CI 5.3-6.1). The risk of very-preterm birth among singletons was 3.6% (n=190); among twins it was 13.2 % (n=225) and among ≥triplets it was 51.8% (n=73) (p<0.0001). We explored whether embryo cryopreservation affected neonatal weight.
For this, we compared the neonatal weight between singletons born after IVF/ICSI with those born after FET, both with autologous oocytes. The mean gestational age of singletons after FET differs considerably from that of fresh embryo transfers, 37.9 and 37.6 WA respectively (p=0.001). Although the difference reached statistical significance, it has no clinical significance, since it only few days. We performed a multivariate lineal regression to determine the effect on neonatal weight. After correcting for gestational age, neonatal weight was not affected by the type of embryo (FET or fresh IVF/ICSI), (coef. -38.8; 95% CI -130.9-53.2, p=0.408). Table 7 shows that perinatal mortality increased significantly with gestational order. Singletons had a perinatal mortality of 6.7 per thousand, compared with 18.5 per thousand in twins and 19.1 per thousands in ≥ triplets (p<0.0001). The RR of perinatal mortality among twins was 2.8 (95% CI 1.9-4.0), and among triplets-and-higher was 2.9 (95% CI 1.4-6.1).
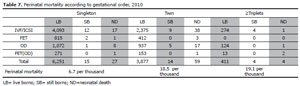
Table 7. Perinatal mortality according to gestational order, 2010
PRE IMPLANTATION GENETIC DIAGNOSIS (PGD)
Clinics located in Argentina, Brazil, Chile, Colombia, Ecuador, México, Panama, Peru, Uruguay and Venezuela reported cycles where PGD and genetic screening (PGS) were performed. Overall, 740 cycles were initiated, and only 480 embryo transfer cycles. The major contributors to 480 transfer cycles were Brazil (55%), Peru (27%) and Argentina (11%). The mean age of women undergoing embryo transfer after PGD was 37 years (21 to 47 years). A mean of six embryos were analyzed in each cycle, and a mean of two of each were reported as normal. 152 clinical pregnancies were registered and 117 deliveries (92 singletons, 24 twins y 1 quadruplet). A total of 144 babies were born after PGD, none of which were reported with any birth defect. After correcting for age of woman, we found no significant effect of PGD on the odds of pregnancy, OR 0.89 (95% CI 0.78-1.02).
MISCARRIAGE RATE
The miscarriage rate in women undergoing IVF/ICSI was 17%, which increased significantly as women age. 13% in women aged ≤34; 18% in women aged 35 through 39 years; 32% in women aged 40 through 42 and 39% in women aged 43 years (p<0.001). The miscarriage rate in women undergoing FET was 22%, and there were no significant differences according to age categories. 21% in women aged ≤34; 23%; in women aged 35 through 39 years; 29% in women aged 40-42 years and 26% in women aged ≥43 (p=0.447). The miscarriage rate in women undergoing OD was 17%, and there were no significant differences according to age categories. 12% in women aged ≤34 years; 17% in women aged 35 through 39 years; 16% in women aged 40-42 and 18% in women aged ≥43 years (p=0.341).
Within each age category, the miscarriage rate did not differ significantly in women having PGD, however, the characteristic of women in each category might be different and therefore, not comparable.
ASSISTED hATChING (Ah)
Clinics in Argentina, Brazil, Mexico, Panama, Peru and Uruguay reported AH in 3,556 embryo transfer cycles, generating 1,162 clinical pregnancies and 892 deliveries (25.1%). Of these, 668 were reported as singletons, 216 twins and 8 triplets. The mean age of the women undergoing assisted hatching was 35 years. After correcting for age, the OR for delivery rate after embryo transfer for AH compared with regular ICSI (no AH), was 1.1 (95% CI 0.98-1.16).
INTRAUTERINE INSEmINATION
Table 8 shows the results of IUI cycles, either with semen of the husband (IIU-H) or donor (IIU-D), reported by clinics located in eight different countries. Forty nine clinics reported 4,874 cycles of IIU-H. The delivery rate per cycles was 15%. The multiple-delivery rate was 14%: 12% twin and 2% triplets-and-higher. Thirty seven clinics reported 876 cycles of IIU-D. The delivery rate per cycles was higher, 20%. The multiple-delivery rate was 13%: 11% twin and 2% triplets-and-higher.
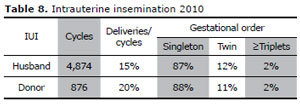
Table 8. Intrauterine insemination 2010
CUMULATIVE/TOTAL DELIVERY RATE
The cumulative delivery rate corresponds to the number of deliveries resulting from one initiated or aspirated ART cycle including the cycle when fresh embryos are transferred, and subsequent frozen/ thawed ART cycles. This rate is used when less than the total numbers of embryos fresh and/or frozen/ thawed have been utilized from one ART cycles. If all embryos are used, it is referred to as total delivery rate. Because this is the first year of a case-by-case registry, cumulative deliveries are calculated by adding deliveries derived from fresh plus frozen transfers. In future years, it will be possible to calculate cumulative events by each person. So far, cumulative delivery rates in Latin America is 28% (Table 9).
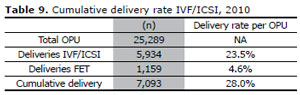
Table 9. Cumulative delivery rate IVF/ICSI, 2010
COMPLICATIONS
Clinics reported 90 cases of ovarian hyper stimulation syndrome, corresponding to a rate of 0.4%. Other less frequent complications included six cases of hemorrhage and one case of infection. It is likely that there is a sub-registry of complications.
DISCUSSION
This is the twenty-first version of the Latin American registry of ART. The RLA has published continuously since 1990, covering ART procedures reported by institutions in Latin America since 1990. Over the years, the RLA has evolved, including the recollection and analysis of more complex information, and allowing the readers to download the resultant in PDF file from our web page (www.redlara.com).
This is the first time we implement a case-by-case register and is the only multinational case-by-case registry. The software used was developed by personnel from the RLA and field-tested in several institutions in the region. In order to implement this new method, workshops were carried out in different countries, and we believe, that the program is still in a developmental phase and continuous check-in systems are being incorporated as problems arise during its implementation. This modification in the reporting system has represented huge demands to all clinics and to personnel working in RLA.
The case-by-case register allowed to simplify the recollection of data, and also, to perform more precise and sophisticated analysis.
Another strength of this register is the uniformity of terminology. All clinics reporting to RLA, use the glossary defined in 2009 by the International Committee for Monitoring Assisted Reproductive Technologies (ICMART) and the World Health Organization (WHO) 1;2. In 2010, 140 clinics from thirteen countries reported the data of 37,853 ART cycles. This represents a small drop of 0.5 % compared to 2009. In 2010 the mean number of cycles registered by each clinic reached 268 cycles, whereas in 2009 it was 281. This drop in the mean number of cycles performed by each clinic can in part result from the lack of public support for infertile couples and therefore, low access to ART procedures3. Only one center from Argentina, which reported 500 cycles in 2009 and one center from Venezuela, which reported 700 cycles in 2009, did not report this year. The rest of centers, which having reported in 2009, did not report in 2010 had only 30 and 150 initiated in 2009. Therefore, it is likely that the number of procedures per center is not increasing as much as new centers reporting.
The use of ICSI instead of conventional IVF continues to increase. In 2010 represented 86% of oocyte pick-ups, while in 2009 and 2008, ICSI represented 85%; and in 2007 the 83% (www.redlara.com). This tendency is also seen in Europe, where in the last report, 69% of autologous cycles were ICSI 4.
The age of women undergoing IVF/ICSI cycles continues to increase. In 2009, the proportion of IVF/ICSI cycles performed in women aged 35 through 39, represented 40%; and 18% of women were ≥40 years. In 2010, women age ≥40 years represent 23% of fresh IVF/ICSI cycles. Furthermore, 7% of IVF/ICSI cycles were performed in women aged ≥43 years. Since the age of the woman is one of the most important prognosis factors, this demographic reality is important to consider when analyzing regional outcomes.
The delivery rate per oocyte pick-up in IVF/ICSI reached 23.4%, and the cumulative delivery rate reached 28%. These results are higher than the data published by ESHRE, where cumulative delivery rate reached 22% 5. Part of this difference is explained by the higher mean number of embryos transferred in Latin America compared with the majority of Europe. The mean number of transferred embryos in IVF/ICSI did not decrease in comparison with previous years. However, the frequency of eSET and eDET did increase significantly. This might be due to a more accurate and thorough register of cases. In spite of this encouraging news, it is worrisome that in 42% of embryo transfers more than three embryos were transferred, and in 7% of cases, more than four embryos were transferred. According to ESHRE´s last report, only 24% of their embryo transfers corresponded to three and more embryos 5.
Both in IVF/ICSI and OD cycles, the transfer of more embryos resulted in an increase in the risk of triplets-and-higher order deliveries. Interestingly, the increase in the risk of twin-deliveries was marginal, and barely reached statistical significance. Thus, 24% of deliveries in IVF/ICSI cycles were multiple (2% triplets-and-higher), and 28% deliveries in OD cycles were multiple (2% triplets and higher). Increasing the number of ET above two, does not significantly impact delivery rates nor twin rates. What it does, is increase the high order multiples which are so detrimental for perinatal mortality and morbidity.
As shown in this as well as previous reports, even twin deliveries increase the risk of preterm birth and perinatal mortality. And as discussed previously, the transfer of ≥two embryos is associated to an increase in the risk of multiple delivery. Probably, the main reason to transfer more embryos is the desire of both clinicians and patients to improve the outcome of each ART cycle, without considering the risk of multiple deliveries and associated prematurity. The data showed in this report is quite reassuring, since the results associated with eSET and eDET, especially in younger patients undergoing IVF/ICSI, and OD cyclesare higher than reported in previous reports.
Since the present report correspond to the analysis of observational data, and not the results of randomized controlled trials, the results cannot be considered as a evidence or support for a decreased benefit in some procedures. For example, PGD was not associated with neither a significant increase in the delivery rate nor a reduction in the miscarriage rate. This might be explained by the fact, that the number of procedures is still low and RLA does not register differently pre-natal genetic diagnosis and pre-natal screening. Furthermore, the selection of women having PGD can be very different to the rest of the population, even when stratified by age. On the other hand, assisted hatching does not increase delivery rate, since no statistical significance was reached, however, caution must be expressed when analyzing this data.
The frequency of complications associated to ART procedures was rather low, only 90 cases of OHSS were reported, which represented a risk of 0.3% of initiated cycles. Furthermore, only 6 cases of genital hemorrhage and 1 case of infections were reported. This might represent a recollection bias, that needs to be improved.
This is the fourth report of IUI cycles. Clinics reported 4,874 IUI with husband´s semen, and 876 cycles with donor´s semen. This represent a clear drop compared to 2009, when 13,410 IIU-H and 2,430 IIU-D cycles were reported. This might be explained by the labor-consuming work that represented the change into a case-by-case register.
In summary, this is the first case-by-case register published by the RLA.
It is reassuring for patients and clinics that the results of ART procedures performed in the region are similar or even better than in most European and Asian countries 6,5. However, REDLARA has to enforce the reduction in the number of embryos transferred in IVF/ICSI and OD cycles, in order to prevent multiple births, or at least, high order multiples and decrease the corresponding perinatal complications.
